📌 Quick Summary
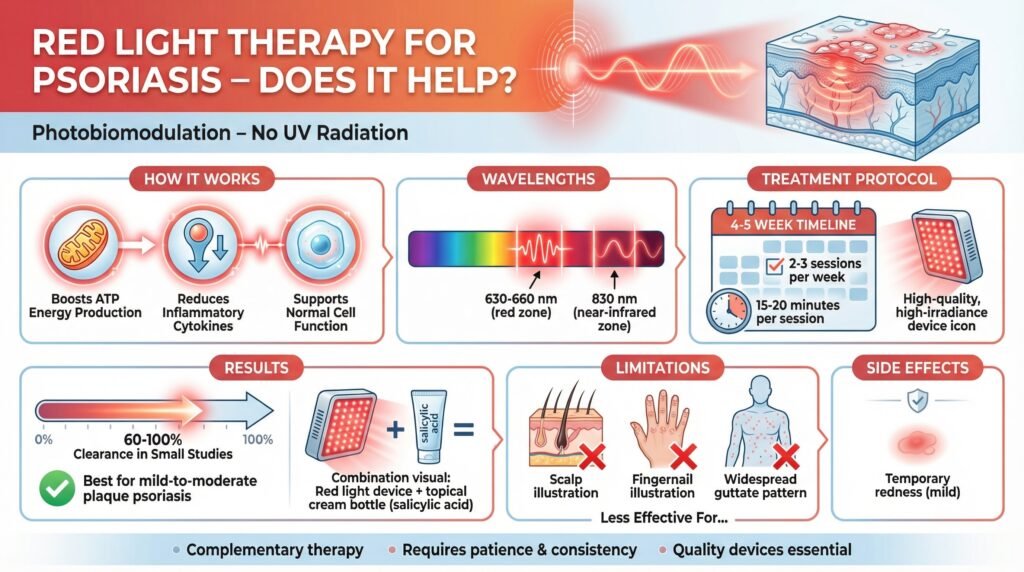
Red light therapy (using 630–660 nm wavelengths, often combined with 830 nm near-infrared) is a safe, non-UV home treatment for psoriasis that works through photobiomodulation: it boosts mitochondrial ATP production, reduces inflammation by modulating cytokines, and supports healthier skin cell function without the cancer risks or immune suppression of traditional therapies.
Research is limited but promising—small studies show 60–100% clearance in some patients after 4–5 weeks of consistent use (2–3 sessions per week, 15–20 minutes each) with quality, high-irradiance devices. It works best as a complementary option for mild-to-moderate plaque psoriasis, especially when combined with topicals like salicylic acid or used for maintenance after UVB. It is less effective for scalp, nail, or widespread guttate psoriasis due to practical limitations. Side effects are minimal (possible temporary redness), but results require patience, consistent high-quality devices, and realistic expectations.
🧾 Table of Contents
- Introduction: Overview of red light therapy as a non-UV, accessible alternative to steroids, medications, and UVB for psoriasis management.
- Understanding Photobiomodulation at the Cellular Level: How red and near-infrared light penetrates the skin, boosts ATP, regulates cell repair, and reduces pro-inflammatory cytokines (unlike UVB’s DNA-damaging mechanism).
- What the Research Actually Shows: Summary of key studies (e.g., 2010 and 2011 trials), clearance rates, protocols used, and limitations of the current evidence.
- Where It Fits Among Your Options Comparison to UVB (gold standard but with cancer risk), PUVA, and medications; best positioning as a low-risk complementary therapy.
- Setting Up Your Treatment Protocol Practical advice: choosing devices (wavelengths, irradiance, panels vs. handheld), session frequency/duration, tracking progress, and improving adherence.
- Adapting for Different Types of Effectiveness and challenges for plaque, guttate, inverse, nail, and scalp psoriasis.
- Combining with Other Treatments: Synergies with salicylic acid, UVB, nutrition, stress management, and other therapies.
- What Can Go Wrong: Potential issues like photosensitivity, Koebner phenomenon, overtreatment, and reasons for lack of results.
- Key Takeaways: Core summary of benefits, requirements, and realistic expectations.
- People Also Asked Answers to common questions (e.g., use with biologics, timeline for results, best wavelengths, comparison to UVB, etc.).
Introduction
Red light therapy for psoriasis has transitioned from a relatively obscure clinical option to something you can now purchase on Amazon and use in your living room while watching Netflix. I’ve watched this evolution with genuine interest, and what strikes me most is how it sits right at the intersection of legitimate dermatology and accessible home treatment.
If you’re dealing with psoriasis, you’ve probably already cycled through the conventional options. Topical steroids that work beautifully for a few months until they suddenly don’t.
Medications with side-effect profiles that make you wonder whether the cure might be worse than the condition.
Light box appointments at your dermatologist’s office twice weekly, where you stand in a booth getting what amounts to a really controlled, really boring tan.
Red light therapy offers something different. Instead of suppressing your immune system or exposing you to UV radiation that carries long-term cancer risks, it works with your body’s natural cellular processes.
And unlike many wellness trends that ask you to believe in quantum vibrations or energy fields, photobiomodulation produces measurable, reproducible effects on mitochondrial function that scientists can actually document and study.
Understanding Photobiomodulation at the Cellular Level
When I first learned about photobiomodulation, I was skeptical. Shining light on your skin to calm down an autoimmune condition sounded suspiciously simple, almost too good to be true.
But the cellular mechanism makes genuine sense once you understand what’s happening.
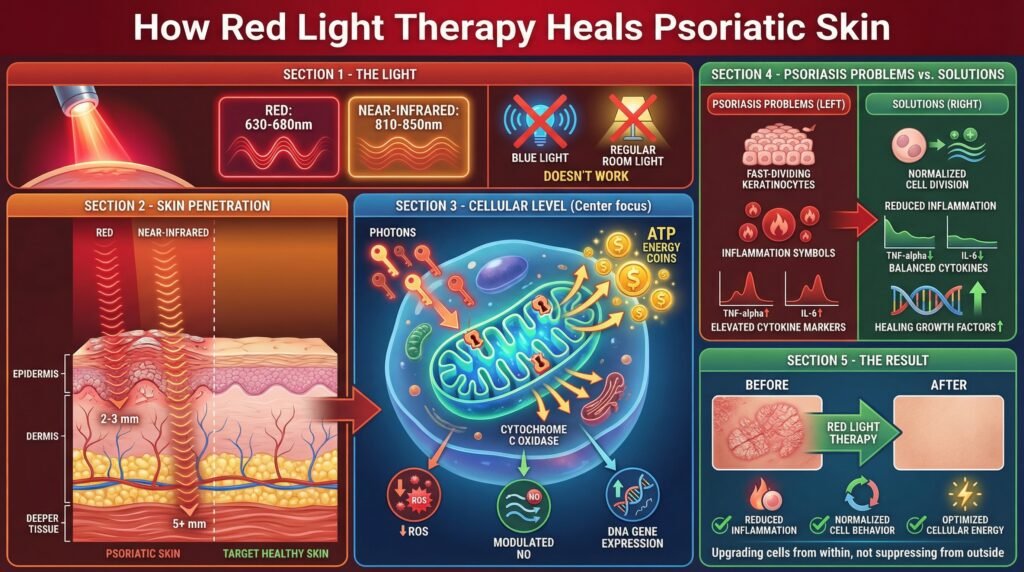
Red light therapy operates in the 620-770 nanometer range. These wavelengths penetrate about six millimeters into your skin, reaching down into the dermal layers where psoriasis inflammation actually develops.
This differs completely from topical treatments that sit on the surface or struggle to penetrate through thick, scaly plaques.
When red light hits your cells, specific chromophores in your mitochondria absorb it, particularly an enzyme called cytochrome c oxidase. This absorption triggers a cascade of cellular events that boost ATP production, essentially giving your cells more energy to perform their normal functions.
For skin cells struggling with the inflammatory chaos of psoriasis, this energy boost helps them regulate better, repair faster, and modulate the inflammatory signals that perpetuate the condition.
Traditional UVB treatment works by slowing down the rapid skin cell turnover that creates those thick, scaly plaques. It does this through controlled DNA damage, therapeutic damage, but damage nonetheless.
Red light therapy takes a completely different approach by supporting normal cellular function rather than disrupting abnormal cell division.
The anti-inflammatory effects happen through cytokine modulation. Psoriasis involves an overactive immune response where certain inflammatory cytokines go into overdrive.
Red light influences macrophages and other immune cells to reduce their production of pro-inflammatory signals like TNF-alpha and interleukins while potentially increasing anti-inflammatory mediators.
Some researchers think combining red light with near-infrared wavelengths around 830 nm might offer synergistic benefits, since each wavelength influences slightly different cellular pathways. The red light handles surface-level inflammation and cellular stimulation, while near-infrared penetrates deeper to affect underlying tissue processes and blood flow.
What the Research Actually Shows
The research on red light therapy for psoriasis is honestly limited compared to established treatments, but what exists is genuinely promising. A 2011 double-blind study compared red light to blue light and found improvements with both after twelve sessions over four weeks.
Blue light performed better specifically for erythema, that angry redness that makes psoriasis so visible, while both wavelengths helped with scaling and thickness.
The most encouraging results came from a 2010 study combining red and near-infrared light. With just nine participants, researchers achieved 60-100% clearance rates over four to five weeks.
Nine people are a really small sample size, and we need to be cautious about extrapolating too much, but those clearance rates are impressive for any psoriasis treatment, especially a non-systemic one.
These studies used clinical-grade equipment in controlled settings. The devices delivered consistent power densities, typically 50-100+ milliwatts per square centimeter, at precise wavelengths.
This matters tremendously when you’re considering at-home devices, many of which don’t provide clear specifications about their actual output or wavelength accuracy.
The typical protocol that emerged involves two to three sessions weekly, each lasting about fifteen to twenty minutes, continued for at least four to five weeks before assessing results. Some protocols included preparatory steps like applying 10% salicylic acid to remove scaling before treatment, potentially improving light penetration into the affected areas.
You’re looking at a meaningful time commitment. Consistency appears to matter more than intensity, which aligns well with what we understand about cellular adaptation and healing processes.
This means actually scheduling sessions and following through, not just buying a device and casually using it whenever you remember.
Where It Fits Among Your Options
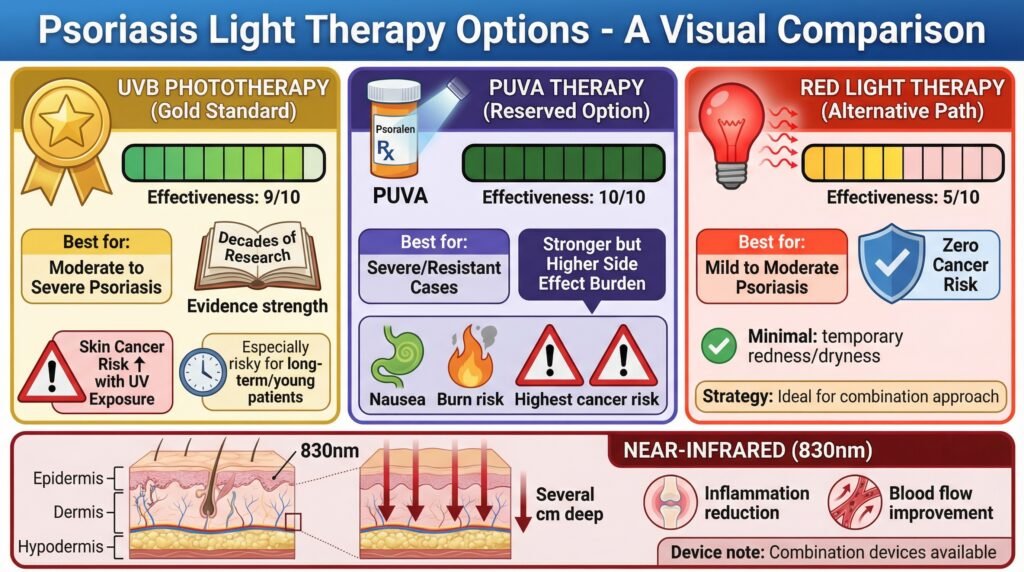
UVB phototherapy remains the gold standard for light-based psoriasis treatment, backed by decades of research and clinical use. It works extremely well for moderate to severe psoriasis, with established protocols and predictable outcomes.
The trade-off is added UV exposure, which increases skin cancer risk over time.
This matters particularly if you’re young or will need long-term management.
PUVA therapy combines psoralen medication with UVA light and works even better for resistant cases, but comes with a higher side effect burden: nausea, increased burn risk, and greater cancer concerns than UVB alone. Dermatologists typically reserve it for severe cases that haven’t responded to other treatments.
Red light therapy sits in a different category entirely. It doesn’t carry the cancer risk of UV exposure, which becomes significant if you’re looking at years or decades of psoriasis management.
The side effects are minimal, occasionally some temporary redness or dryness that resolves quickly.
But the evidence of effectiveness is substantially weaker than established phototherapy options.
This creates an interesting decision point for people with mild to moderate psoriasis who want to avoid medications but aren’t willing to accept the UV exposure of traditional phototherapy. Red light becomes a reasonable option, particularly as part of a combination approach rather than monotherapy.
Near-infrared light at 830 nm penetrates even deeper, up to several centimeters into tissue. While psoriasis is primarily a skin surface condition, the deeper penetration might influence underlying inflammatory processes and blood flow in ways that support healing.
Some combination devices offer both wavelengths, theoretically providing complementary benefits.
Setting Up Your Treatment Protocol
Starting with red light therapy requires more strategic thinking than just purchasing the first device you find. I recommend beginning with a clear baseline assessment.
Take detailed photographs of affected areas in consistent lighting, preferably natural indirect sunlight.
Document specific measurements of plaque size and thickness.
This documentation matters because psoriasis fluctuates naturally. Without baseline photos, you really can’t tell whether the changes you’re seeing are treatment effects or just normal variation.
Device selection deserves serious attention. The market is flooded with “red light therapy” products making broad wellness claims without specific dermatological applications.
Look for devices that specify their wavelength output.
You want something in the 630-660 nm range for red light, potentially combined with 830 nm near-infrared.
Power density specifications matter tremendously. Devices should provide irradiance measurements in mW/cm², allowing you to calculate suitable treatment times.
FDA clearance for dermatological applications provides some quality assurance, though what’s more important is whether the device has published clinical data or has been used in actual research studies.
Consumer reviews can be helpful, but take them with suitable skepticism. Psoriasis responds to placebo effects, and people’s enthusiasm for products they’ve invested in creates bias.
Look for specific details about wavelengths, power output, and treatment area coverage rather than general enthusiasm about results.
Treatment area coverage affects practicality significantly. If your psoriasis affects large body areas, handheld devices become tedious quickly.
Panel-style devices covering larger areas make consistent treatment more possible, which matters enormously for adherence.
The Pennsylvania LITE study on home phototherapy found patients were three times more likely to maintain prescribed frequency with convenient home setups compared to in-office treatments.
Start with the protocol supported by research. Two to three sessions weekly, fifteen to twenty minutes per area, maintained consistently for at least four weeks before assessing effectiveness.
Position the device according to the manufacturer’s specifications regarding distance.
Light intensity follows the inverse square law, so small distance changes significantly affect dose delivery.
Weekly photographs from identical angles in consistent lighting reveal changes you might miss when looking at your skin daily. Some people track subjective measures too: itching intensity, flaking, comfort levels.
These capture quality-of-life improvements that photographs might miss.
Adapting for Different Types
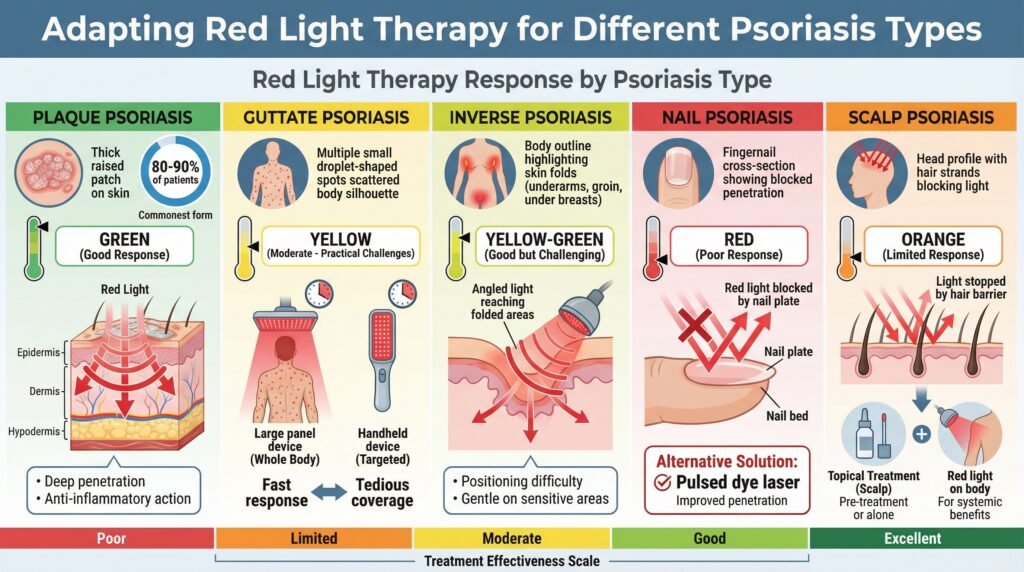
Plaque psoriasis, affecting about 80-90% of psoriasis patients, responds reasonably well to red light therapy in research settings. The thick, raised plaques benefit from red light’s deeper penetration, and the anti-inflammatory effects address the underlying immune dysfunction driving plaque formation.
Guttate psoriasis presents different challenges. The smaller, drop-like lesions scattered across the body mean covering all affected areas needs either larger panel devices or significantly more treatment time.
The thinner lesions might actually respond faster than thick plaques, but the practicality of treating many small spots becomes tedious.
Inverse psoriasis, occurring in skin folds like under the breasts or in the groin, creates positioning challenges for light delivery. These areas are also more sensitive and prone to irritation, though red light’s gentle nature actually works well here compared to harsher topical treatments.
Nail psoriasis typically doesn’t respond well to red light therapy. The nail plate blocks light penetration to the affected nail bed and matrix.
Pulsed dye lasers show much better results for nail psoriasis, targeting the blood vessels contributing to nail changes with wavelengths specifically absorbed by hemoglobin.
For scalp psoriasis, red light therapy faces hair interference, blocking light from reaching the scalp. Some people find that handheld devices work along part lines and can reach affected areas, but this becomes time-consuming with extensive scalp involvement.
Combination approaches using topical treatments to manage scalp psoriasis while using red light for body lesions often work better.
Combining with Other Treatments
Salicylic acid preparation before red light sessions serves a really practical purpose. Thick scaling blocks light penetration, reducing how much actually reaches the deeper skin layers where it can work.
Removing that barrier with keratolytic agents potentially improves treatment efficacy, though this hasn’t been rigorously studied.
Some practitioners strategically mix red light with traditional UVB phototherapy, starting with more aggressive UVB to achieve initial clearance, then transitioning to maintenance with red light to minimize added UV exposure.
This approach lacks formal research support but makes theoretical sense for long-term management.
Anti-inflammatory nutrition, stress management, and adequate sleep all influence psoriasis activity through various mechanisms. Red light therapy works synergistically with these foundational approaches rather than replacing them.
What Can Go Wrong
Red light therapy’s safety profile is genuinely impressive, but a few considerations deserve attention. Photosensitizing medications can create problems even with non-UV light.
If you’re taking drugs like certain antibiotics, NSAIDs, or even some herbal supplements, they can increase your skin’s reactivity to light exposure.
Most photosensitizing concerns focus on UV wavelengths, but understanding your medication profile before starting any light therapy makes sense.
The Koebner phenomenon, where new psoriasis lesions develop at sites of skin trauma, affects some people with psoriasis. While red light therapy is gentle and non-traumatic, some people develop new lesions in treated areas.
This is rare but worth monitoring, particularly in the first few weeks of treatment.
Overtreatment can still cause problems even though red light therapy is gentler than UV therapy. Excessive light exposure might trigger paradoxical inflammation or simply waste time without extra benefits.
The dose-response relationship for photobiomodulation follows a biphasic curve: too little doesn’t work, optimal dosing produces benefits, but excessive exposure often reduces returns or even reverses benefits.
Eye protection deserves consideration depending on device type and treatment areas. While red and near-infrared light don’t carry the same acute eye damage risks as UV, high-intensity LEDs directed toward the face warrant protective eyewear.
Most manufacturers provide guidance on this.
Realistic timeframe expectations prevent premature abandonment of treatment. Psoriasis responds slowly to most interventions, and red light therapy is no exception.
Meaningful improvement typically needs four to five weeks of consistent treatment, longer than many people’s patience extends, especially with at-home treatments lacking professional accountability.
Key Takeaways
Red light therapy for psoriasis represents a legitimate treatment option with sound biological mechanisms and promising early research, though evidence remains limited compared to established therapies. The treatment stimulates mitochondrial ATP production and modulates inflammatory cytokines rather than causing DNA damage like UV phototherapy.
Clinical studies show 60-100% clearance rates in small trials using combined red and near-infrared wavelengths over four to five weeks with consistent treatment. These results come with important caveats about small sample sizes and clinical-grade equipment that may not reflect at-home device performance.
Effective implementation needs specific wavelengths in the 630-660 nm red range, optionally combined with 830 nm near-infrared, adequate power density of 50-100+ mW/cm², consistent frequency of two to three sessions weekly, and realistic timeframes of four to five weeks at least before assessing results.
Red light therapy works best as part of combination approaches, complementing topical treatments, lifestyle modifications, or even traditional phototherapy in strategic protocols that minimize UV exposure while maintaining effectiveness.
The safety profile is favorable with minimal side effects, no cancer risk, and rare complications limited primarily to interactions with photosensitizing medications or unusual Koebner phenomenon responses in susceptible people.
Success needs systematic documentation, consistent adherence maintained over weeks rather than days, suitable device selection with verified specifications, and integration with comprehensive psoriasis management rather than reliance on red light therapy alone.
People Also Asked
Does red light therapy work for psoriatic arthritis?
Red light therapy hasn’t been specifically studied for psoriatic arthritis, though some people report joint pain improvement. The anti-inflammatory effects that help skin lesions might theoretically benefit inflamed joints, but near-infrared wavelengths penetrate deeper and show more promise for joint conditions than red light alone.
Standard treatments for psoriatic arthritis stay more evidence-based options.
How long does it take to see results from red light therapy for psoriasis?
Most clinical studies showed improvement after four to five weeks of consistent treatment at two to three sessions weekly. Some people notice reduced itching or inflammation within two weeks, but visible plaque reduction typically takes longer.
Expecting results before four weeks often leads to premature discontinuation.
Can I use red light therapy with biologics for psoriasis?
Red light therapy and biologics work through different mechanisms and shouldn’t interfere with each other. Biologics target specific immune pathways systemically, while red light provides local cellular effects.
However, you should talk about any treatment additions with your dermatologist, particularly if you’re on medications that affect your immune system or cause photosensitivity.
What wavelength is best for psoriasis treatment?
Clinical studies showing the best results used red light in the 630-660 nm range, often combined with near-infrared at 830 nm. The red wavelengths handle surface inflammation and cellular stimulation, while near-infrared penetrates deeper for extra anti-inflammatory effects.
Avoid devices that don’t specify exact wavelengths, as this information is critical for effectiveness.
Is red light therapy better than UVB for psoriasis?
UVB phototherapy has substantially more research supporting its effectiveness and remains the gold standard for light-based psoriasis treatment. Red light therapy offers the advantage of no UV exposure and, therefore, no cancer risk, making it attractive for long-term management.
For severe psoriasis, UVB typically produces more reliable clearance.
Can red light therapy cause psoriasis to flare?
Red light therapy rarely causes psoriasis flares, though some people with active Koebner phenomenon might develop new lesions in treated areas. This differs from UV therapy, which can sometimes trigger flares if dosing is too aggressive.
Most people tolerate red light therapy well without worsening symptoms.
Do cheap red light devices work for psoriasis?
Device quality matters tremendously for psoriasis treatment. Many inexpensive devices don’t provide adequate power density, accurate wavelengths, or enough coverage area.
Look for devices with published specifications showing at least 50 mW/cm² irradiance at verified wavelengths in the 630-660 nm range.
Clinical studies used professional-grade equipment, not consumer wellness devices.
Should I stop my psoriasis medication to try red light therapy?
Never stop prescribed psoriasis medications without consulting your dermatologist. Red light therapy works best as a complementary treatment rather than a replacement for established therapies.
Many people use it alongside topical treatments or to reduce medication frequency once they achieve improvement, but these decisions should involve your healthcare provider.
This article includes affiliate links. If you click through and make a purchase, I may receive a small commission. This helps support the site and allows me to keep creating helpful content at no extra cost to you.