📌Quick Summary: Fast Facts
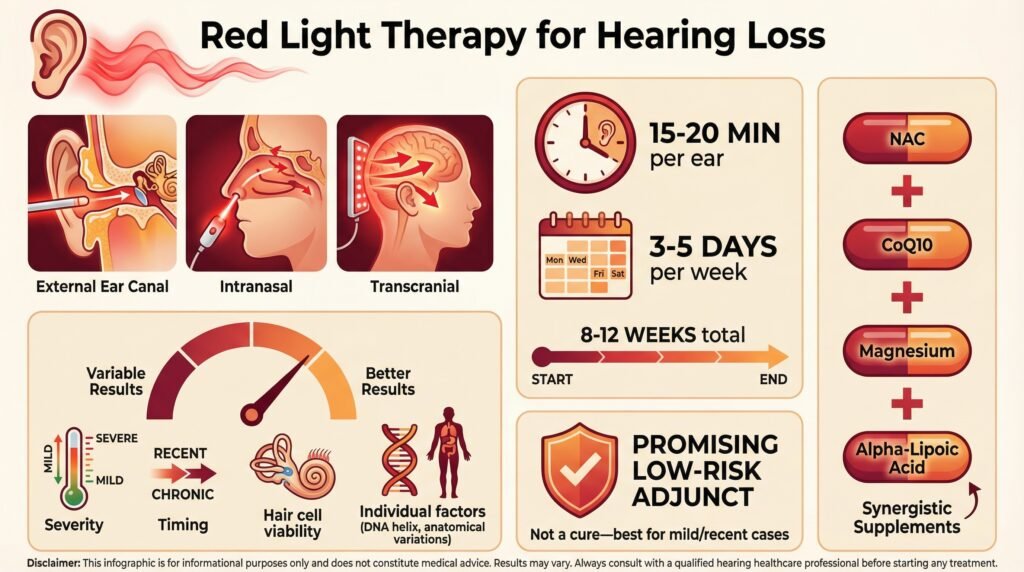
Different red light application methods (external ear canal, intranasal, transcranial), optimal session durations and frequencies (typically 15–20 minutes per ear, 3–5 times per week for 8–12 weeks), device recommendations, synergistic use with supplements like NAC, CoQ10, magnesium, and alpha-lipoic acid, are necessary for adequate results
There is significant individual variability in results based on hearing loss severity, cause, anatomy, and genetics, and stresses that benefits are most likely in milder or recent cases where some viable hair cells remain. Overall, it presents red light therapy as a promising, low-risk adjunct rather than a cure, with practical self-treatment guidance and key takeaways.
In part 1 of this series, we covered understanding photobiomodulation in the auditory system, the different types of hearing loss, and touched upon some red light treatment protocols. In part 2, we discuss treatment protocols, combining interventions, and expand on more at-home red light therapy devices you can use to help with treating hearing loss. Follow us for additional updates and educational content.
🧾 Table of Contents
· Treatment Protocols and Technical Considerations (Continued)
- Application Methods (External ear canal, intranasal, transcranial, and experimental surgical approaches)
- Treatment Duration and Frequency (Acute vs. chronic protocols, session length of 10–30 minutes)
- Best Red Light Therapy Devices for Hearing Loss / Tinnitus (Panels like Hooga and MitoRed, handheld wands like LightStim and Quasar MD Plus)
· Combining Red Light Therapy with Other Interventions (Synergistic effects with antioxidants such as NAC, CoQ10, magnesium, alpha-lipoic acid; sound therapy, auditory training, and hearing aids)
· Understanding Individual Response Variability (Factors including cause/severity of hearing loss, tissue optics, ear anatomy, middle ear conditions, and genetics)
· Practical Self-Treatment Approaches
· Key Takeaways
· People Also Asked (Common questions: timeline for improvement, light penetration to the inner ear, and safety for ears)
Treatment Protocols and Technical Considerations (Continued)
Application Methods
The location and method of light application matter more than you might think. Several approaches have been explored in research settings, each with advantages and limitations.
External ear canal application is the most practical for clinical use. A light-emitting probe is positioned at the entrance to the ear canal, allowing light to travel down the canal toward the tympanic membrane.
Some light will reflect off the eardrum, but some passes through it into the middle ear space and potentially reaches the cochlea.
The obvious advantage of this approach is that it’s non-invasive and simple to implement. The disadvantage is that there are legitimate questions about how much light actually reaches the cochlea through all the intervening structures, the tympanic membrane, middle ear bones, and cochlear bone.
Intranasal application is an interesting choice that some researchers have explored. The nasal cavity shares blood supply with the inner ear through the internal carotid artery system. By applying light intranasally, you may be able to influence cochlear function through systemic effects on blood flow and cellular signaling, even if the light itself doesn’t directly reach the cochlea.
Transcranial application, where light is applied to the skin over the temporal bone, is another approach. Near-infrared wavelengths can penetrate several centimeters through tissue and bone, potentially reaching the cochlea.
This method avoids the ear canal entirely but needs higher power to deliver adequate energy to the target tissue.
In research settings, some highly experimental approaches have involved surgical placement of light-emitting devices directly near the cochlea. This obviously maximizes light delivery to the target tissue, but it needs surgery and isn’t practical for clinical application.
Treatment Duration and Frequency
Treatment duration and frequency vary widely across studies, making it difficult to identify a single optimal protocol. The best approach likely depends on what condition you’re treating and whether you’re trying to prevent damage, address acute injury, or manage chronic conditions.
For acute noise damage, intensive short-term treatment appears most effective. Some animal studies have used treatments immediately after noise exposure, then daily for 3-5 days.
This aggressive early intervention targets the critical period when secondary damage is unfolding.
For chronic conditions like age-related hearing loss or tinnitus, sustained regular treatments seem necessary. Most human studies showing benefits have used protocols involving 3-5 treatments per week for at least 8-12 weeks.
Some evidence suggests that maintenance treatments, perhaps once or twice weekly, may help sustain benefits after an initial intensive course.
Session duration typically ranges from 10-30 minutes per ear. Longer treatments deliver more total energy and increase the risk of adverse effects from heat buildup or excessive stimulation.
Most researchers have settled on 15-20 minute sessions as a reasonable compromise.
Best Red Light Therapy Devices for Hearing Loss / Tinnitus
Although not specifically designed for the ears, Red light panels from brands such as Hooga Health and MitoRedLight provide similar, targeted therapeutic near-infrared light for improving circulation to the ear, as well as providing the flexibility of expanding to larger parts of the body.
As mentioned in part 1, targeted handheld wands such as the Lightstim and the Quasar MD Plus are affordable, low-EMF devices that can be used for close, focused application to the ear canal and outer ear.
Typically designed for the targeted face and neck treatments, these devices provide the efficacious wavelengths of around 660nm for the surface tissue and near-infrared light of around 850 nm to penetrate deeper into the skin. Read our reviews of the FDA-cleared Lightstim here and the Quasar MD Plus hand-held device here.
>>Click here to buy the Lightstim Handheld Device on Amazon<<
>>Click here to buy the Quasar MD Plus<<
Combining Red Light Therapy with Other Interventions
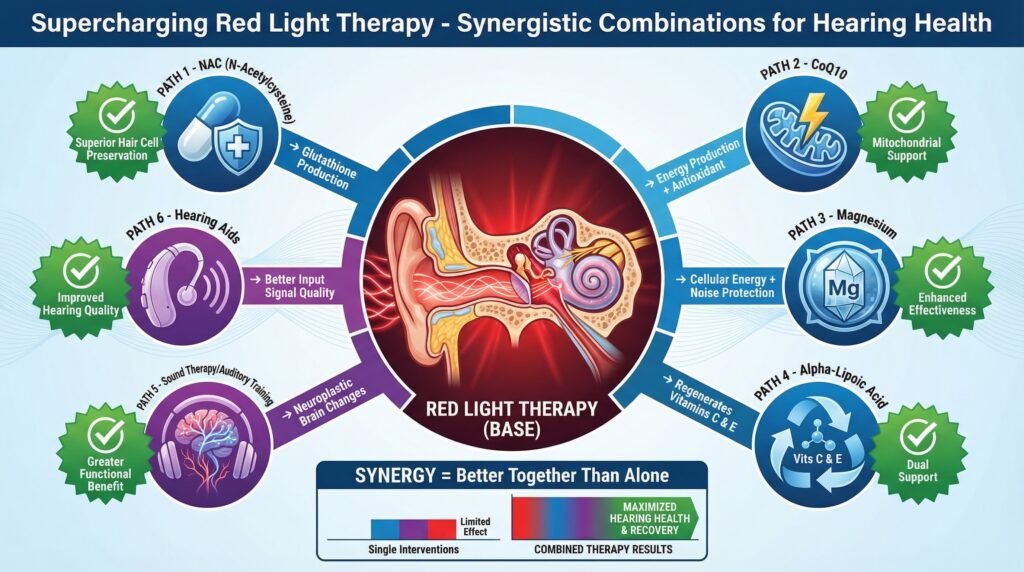
One of the most promising aspects of photobiomodulation is that it appears to work synergistically with other protective and therapeutic interventions. Research has shown enhanced benefits when red light therapy is combined with strategies that complement its mechanisms.
Antioxidant supplementation makes logical sense as a complementary intervention. If photobiomodulation works partly by reducing oxidative stress and supporting mitochondrial function, combining it with nutrients that serve similar functions should amplify the effects.
N-acetylcysteine (NAC) is a precursor to glutathione, the body’s primary antioxidant. Multiple studies have shown that NAC can reduce noise-induced hearing loss when taken before and after acoustic trauma.
Some animal research has demonstrated that combining NAC with photobiomodulation provides significantly better hair cell preservation than either intervention alone.
Coenzyme Q10 (CoQ10) is a mitochondrial cofactor involved in electron transport and also functions as an antioxidant. CoQ10 supplementation has shown some benefit for age-related hearing loss in human studies.
Using CoQ10 alongside photobiomodulation could support mitochondrial function through complementary mechanisms.
Magnesium plays important roles in both auditory function and cellular energy production. Magnesium deficiency increases vulnerability to noise damage, and supplementation has shown protective effects.
Combining adequate magnesium intake with photobiomodulation could enhance the therapy’s effectiveness.
Alpha-lipoic acid is both a mitochondrial cofactor and a powerful antioxidant that can regenerate other antioxidants like vitamin C and E. Some research suggests benefits for tinnitus and noise-induced hearing loss.
Using alpha-lipoic acid with photobiomodulation could provide complementary mitochondrial support and antioxidant protection.
Sound therapy and auditory training might also complement photobiomodulation through different mechanisms. While red light therapy works at the cellular and metabolic level in the cochlea, auditory training can promote neuroplastic changes in how the brain processes auditory information.
For someone with hearing loss, improving the health of existing hair cells through photobiomodulation while simultaneously training the auditory system to more efficiently process the signals those cells send could theoretically provide greater functional benefit than either approach alone.
Even conventional interventions like hearing aids might work better in conjunction with photobiomodulation. If the therapy can preserve or even slightly improve the function of remaining hair cells, hearing aids would have better input signals to amplify, potentially improving overall hearing quality and reducing the degree of amplification needed.
Understanding Individual Response Variability
One of the frustrating aspects of current red light therapy research for hearing loss is the significant variability in person responses. Some people experience measurable improvements in hearing thresholds, some notice subjective benefits without objective changes, and others see no effect at all.
The underlying cause and severity of hearing loss clearly influence treatment response. Someone with recent noise-induced damage to hair cells that are still viable but stressed might respond very differently from someone with decades of accumulated damage and significant hair cell loss.
You can’t regenerate cells that no longer exist, and photobiomodulation can’t restore function to structures that have been destroyed.
A person with mild hearing loss (20-40 decibel threshold elevation) has more remaining functional hair cells than someone with severe hearing loss (70+ decibel threshold elevation). Those remaining cells are the substrate that photobiomodulation works with, so people with milder loss simply have more potential for improvement.
Individual differences in tissue optical properties also play a significant role in how much light actually reaches the cochlea. Skin pigmentation affects light absorption, with darker skin absorbing more light in the red spectrum.
Ear canal anatomy varies between people, influencing how well light can travel down the canal.
Some people have narrower canals or more pronounced curves that may reduce light transmission.
The thickness and properties of the tympanic membrane vary between people and can change with age or a history of ear infections. A thicker, more opaque eardrum will send less light to the middle ear than a thin, translucent one.
Middle ear conditions can dramatically affect light transmission. Someone with chronic middle ear inflammation, fluid accumulation, or significant earwax buildup might receive substantially less effective light delivery than someone with clear, healthy middle ear structures.
Genetic factors related to mitochondrial function, antioxidant enzyme activity, and cellular repair mechanisms could influence how well someone’s cochlear cells respond to photobiomodulation. We’re just beginning to understand the genetic components of hearing loss susceptibility and recovery capacity.
For example, variations in genes encoding antioxidant enzymes like superoxide dismutase or glutathione peroxidase might affect how well someone’s cochlear cells handle oxidative stress. Someone with genetically more robust antioxidant systems might respond differently to photobiomodulation than someone with less efficient systems.
Lifestyle factors also matter. Smoking impairs blood flow and increases oxidative stress throughout the body, including in the cochlea.
Someone who smokes might respond less well to photobiomodulation than a non-smoker because the ongoing oxidative burden counteracts the therapy’s benefits.
Nutritional status influences mitochondrial function and cellular repair capacity. Someone with deficiencies in key nutrients like B vitamins, magnesium, or coenzyme Q10 might not respond as well as someone with optimal nutritional status.
Practical Self-Treatment Approaches
While much of the research involves specialized medical devices, consumer-grade red light therapy devices have become widely available. This raises the question of whether effective self-treatment at home is realistic.
The answer depends heavily on understanding both the possibilities and limitations.
First, recognize that most consumer devices weren’t specifically designed for auditory applications. They’re typically made for skin rejuvenation, wound healing, or general wellness purposes.
That doesn’t mean they can’t potentially work for hearing-related applications, but you’ll need to assess carefully whether a particular device is suitable.
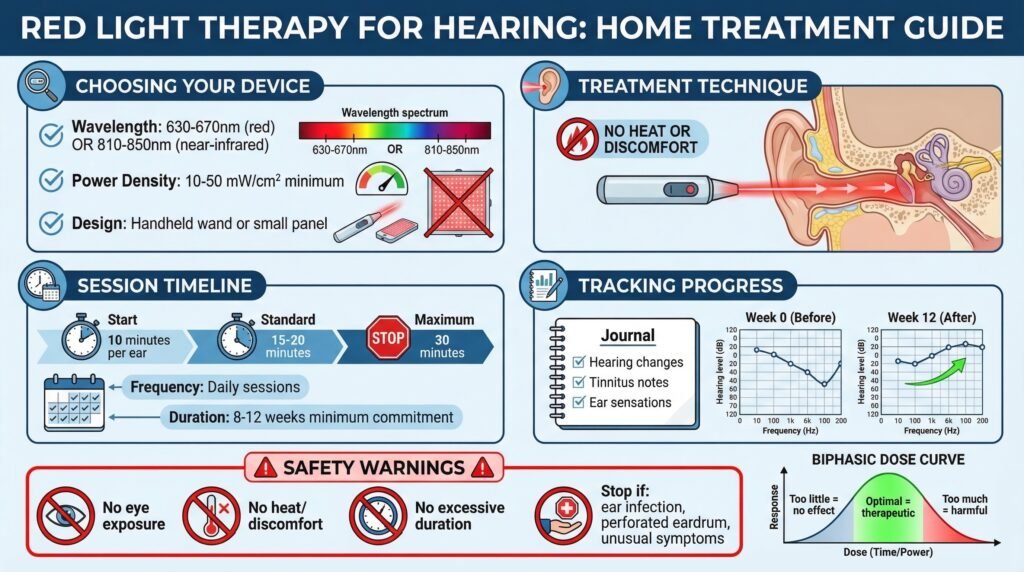
Look for devices that emit wavelengths in the therapeutic range for photobiomodulation. Ideally, you want red light around 630-670 nm or near-infrared around 810-850 nm.
Many devices provide this information in their technical specifications.
Avoid devices that only specify “red light” without giving specific wavelength information.
The device should have sufficient power output to deliver therapeutic energy doses. Very low-power devices designed for cosmetic use may not provide adequate intensity for deeper tissue effects.
Look for devices specifying power density in the range of at least 10-50 milliwatts per square centimeter.
The device needs to be designed in a way that allows you to position it safely near or at the entrance to your ear canal. Handheld wands or small panels work better for this application than large flat panels designed for treating broad areas of skin.
The treatment technique needs some care. Position the light source at the entrance to the ear canal without inserting anything into the canal itself.
The goal is to allow light to enter the canal and travel toward the eardrum.
You should never experience heat or discomfort during treatment. If you do, the device is too powerful or positioned too close.
Start with modest session durations, perhaps 10 minutes per ear, and gradually increase if you tolerate it well without any adverse effects. Most research protocols have used 15-20 minute sessions.
Going much beyond 30 minutes doesn’t appear to provide additional benefits and might risk adverse effects.
Consistency matters far more than any single session. Sporadic treatment is unlikely to produce meaningful results.
Plan for daily or near-daily sessions for at least 8-12 weeks before deciding whether the intervention is helping.
Monitor your response systematically as opposed to relying on vague impressions. Keep a journal noting any changes in hearing ability, specific situations where you notice differences, tinnitus characteristics if relevant, and any ear sensations.
Over weeks of treatment, you might notice gradual improvements that would be hard to detect without systematic tracking.
If you’re going to try self-treatment seriously, get a baseline audiogram before starting and follow-up testing after 8-12 weeks of consistent treatment. This gives you objective data as opposed to just subjective impressions, which can be influenced by placebo effects and wishful thinking.
Safety should be your absolute priority. Never use devices that produce heat or discomfort.
Don’t use excessively powerful devices or extend session times beyond recommended durations, thinking that more is better.
Photobiomodulation follows a biphasic dose response where too much can be counterproductive or even harmful.
Never shine light directly at your eyes. While red and near-infrared light at suitable intensities won’t damage your eyes the way lasers can, unnecessary exposure should still be avoided.
Be cautious if you have any active ear infections, perforated eardrums, or unusual ear symptoms. Get a medical evaluation for these conditions before attempting any self-treatment with light therapy.
Key Takeaways
Red light therapy shows genuine promise for certain types of hearing loss, particularly noise-induced damage, age-related decline, and some cases of tinnitus. The therapy works primarily through enhanced mitochondrial function and reduced oxidative stress in cochlear cells.
Treatment parameters matter enormously. Wavelength, power density, duration, and frequency of sessions all significantly impact outcomes, with most research supporting wavelengths between 630-850 nm and sessions of 10-20 minutes.
The timing of intervention is critical for acute hearing damage. The best protective effects occur when photobiomodulation is applied within hours to days of noise exposure or sudden hearing loss.
Individual responses vary substantially based on the underlying cause of hearing loss, severity of damage, tissue optical properties, and possibly genetic factors affecting cellular repair capacity.
Combining photobiomodulation with other interventions like antioxidant supplementation and auditory training may provide synergistic benefits beyond any single approach.
Realistic expectations are essential. This therapy can potentially preserve function, provide modest improvements, and slow progression, but cannot regenerate destroyed hair cells or reverse decades of severe damage.
Systematic monitoring through audiometry, speech discrimination testing, and careful subjective tracking is necessary to decide whether treatment is actually effective for your specific case.
People Also Asked
How long does it take for red light therapy to improve hearing?
The timeline for potential hearing improvement with red light therapy varies considerably depending on the type and severity of hearing loss. For acute noise-induced damage, protective effects may be measurable within days to weeks when treatment begins shortly after exposure.
For chronic conditions like age-related hearing loss or tinnitus, most studies showing benefits have used treatment protocols lasting 8-12 weeks with many sessions per week.
Some people notice subjective improvements in hearing or tinnitus within 4-6 weeks, while others need longer treatment courses. Measurable changes on audiometry typically appear after at least 8 weeks of consistent treatment.
For chronic conditions, maintenance treatments may be needed to sustain benefits.
Can red light penetrate to the inner ear?
Red and near-infrared light can penetrate through skin, soft tissue, and even bone to reach deeper structures, though the amount that reaches the inner ear depends on several factors. Near-infrared wavelengths around 810-850 nm penetrate more effectively than shorter red wavelengths.
Light can travel down the ear canal, pass through the tympanic membrane, traverse the middle ear space, and potentially reach the cochlea.
However, the percentage of applied light that actually reaches the cochlear hair cells is reduced by absorption and scattering through these structures. Research using transcranial application has demonstrated that near-infrared light can penetrate through the temporal bone to reach the cochlea when sufficient power is used.
Is photobiomodulation safe for the ears?
Photobiomodulation using suitable parameters appears to be safe for auditory applications based on current research. Studies in both animals and humans have not reported significant adverse effects when proper wavelengths, power densities, and treatment durations are used. The therapy does not involve ionizing radiation and doesn’t cause tissue damage when applied correctly.
The main safety considerations are avoiding excessive heat buildup, which can occur with too much power or overly long treatment times, and not using the therapy if you have active ear infections or perforated eardrums.
Professional guidance is recommended to confirm suitable treatment parameters, and you should stop treatment if you experience any pain, increased hearing loss, or unusual symptoms. Get started with a reliable and affordable handheld red light device today.
This article includes affiliate links. If you click through and make a purchase, I may receive a small commission. This helps support the site and allows me to keep creating helpful content at no extra cost to you.