📌Quick Summary: Fast Facts
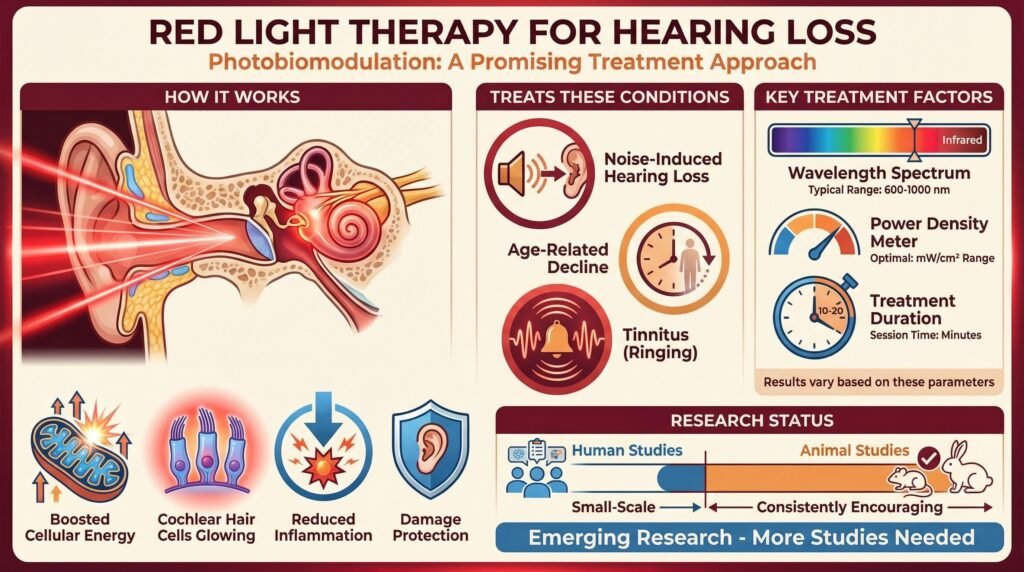
- Red light therapy (photobiomodulation) shows promise in treating certain types of hearing loss by stimulating cellular energy production in the delicate structures of the inner ear.
- Studies show potential benefits for noise-induced hearing loss, age-related hearing decline, and tinnitus, though results vary significantly based on wavelength, power density, and treatment duration.
- The therapy works by enhancing mitochondrial function in cochlear hair cells, reducing inflammation, and potentially protecting against further auditory damage.
- Current research is still emerging, with most human studies being small-scale, though animal models have shown consistently encouraging results.
🧾 Table of Contents
· Introduction
· Understanding Photobiomodulation in the Auditory System
· The Evidence for Different Types of Hearing Loss
- Noise-Induced Hearing Loss
- Age-related hearing loss
- Tinnitus
· Treatment Protocols and Technical Considerations
- Wavelength Selection
- Power Density and Energy Dose
- Best Red Light Therapy Devices for Hearing Loss / Tinnitus
· People Also Asked
- Does red light therapy work for tinnitus?
- Can hearing loss from loud noise be reversed?
- What wavelength of red light is best for hearing?
- How long does it take for red light therapy to improve hearing?
Introduction
I’ll admit that when I first encountered the idea of shining light into ears to improve hearing, I was pretty skeptical. It sounded like something from a science fiction novel as opposed to legitimate medical research.
But after digging into the actual science behind photobiomodulation and its effects on auditory function, I’ve come to appreciate just how fascinating and potentially transformative this therapy could be for people struggling with hearing loss.
The inner ear is one of the most metabolically active tissues in the entire human body. Those tiny hair cells that translate sound vibrations into neural signals need enormous amounts of cellular energy to function properly.
When they’re damaged, whether from loud noise exposure, aging, medications, or disease, the consequences are often permanent because mammalian hair cells don’t regenerate.
Or at least, they don’t regenerate naturally. This is where red light therapy comes in, and the mechanism is quite elegant.
Understanding Photobiomodulation in the Auditory System
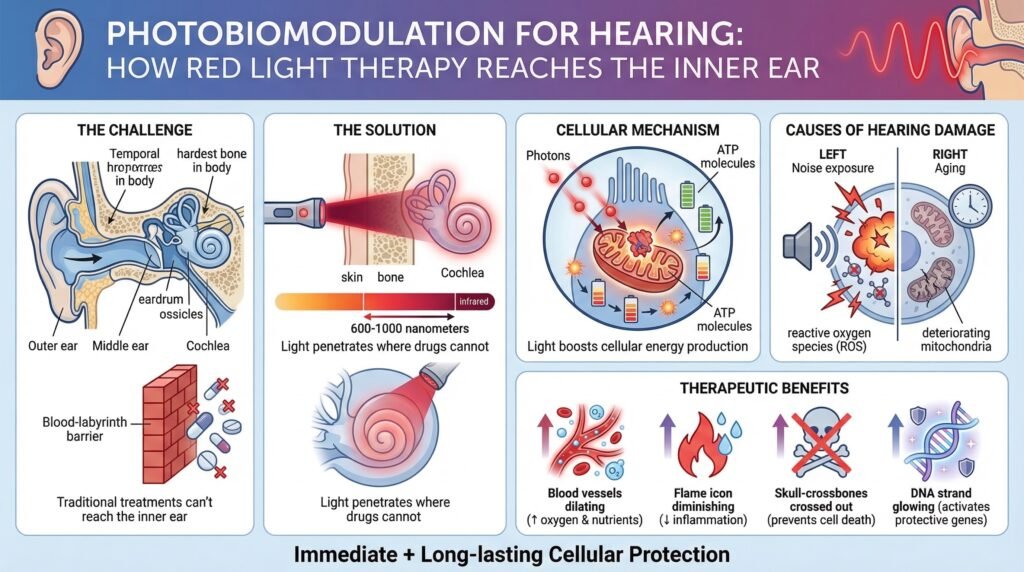
The inner ear presents a unique challenge for therapeutic interventions. The cochlea is encased in the hardest bone in the human body, filled with fluid, and contains some of the most delicate cellular structures we possess.
Traditional drug delivery to this area is notoriously difficult because of the blood-labyrinth barrier that restricts what substances can reach the inner ear.
Oral medications must pass through many barriers, and even intratympanic injections (medications placed directly in the middle ear) face limitations in how well they penetrate to the cochlea.
Light, however, can penetrate tissues in ways that medications cannot. Specific wavelengths in the red to near-infrared spectrum (typically between 600-1000 nanometers) can pass through skin, bone, and other tissues to reach deeper structures.
What makes this particularly relevant for hearing is that these wavelengths interact with specific molecules in our cells in really useful ways.
Photobiomodulation works primarily through the absorption of light by chromophores in our cells. The most important of these is cytochrome c oxidase, an enzyme in the mitochondrial respiratory chain. Mitochondria are the power plants of our cells, responsible for producing ATP, the energy currency that powers all cellular processes.
When cytochrome c oxidase absorbs photons in the red to near-infrared spectrum, it undergoes subtle structural changes that make it more efficient at facilitating electron transfer. This enhanced electron transport leads directly to increased ATP production.
For hair cells that are struggling because of damage or metabolic stress, this boost in energy production can mean the difference between survival and death.
What makes this particularly relevant for hearing loss is that many forms of auditory damage involve oxidative stress and mitochondrial dysfunction. Noise exposure doesn’t just mechanically damage hair cells through excessive vibration.
The loud sound creates a cascade of reactive oxygen species that continues to harm cells for hours or even days after the initial acoustic trauma.
These free radicals damage cellular membranes, proteins, and DNA, leading to cellular dysfunction and death.
Age-related hearing loss similarly involves progressive mitochondrial decline. As we age, our mitochondria accumulate damage, produce less ATP, and generate more reactive oxygen species.
The cochlear hair cells, being so metabolically demanding, are particularly vulnerable to this age-related mitochondrial deterioration.
Red light therapy interrupts these destructive processes while simultaneously supporting cellular repair mechanisms. Research has shown that photobiomodulation can increase blood flow to the cochlea by triggering vasodilation.
Better blood flow means more oxygen and nutrients reach the hair cells, while metabolic waste products are removed more efficiently.
The therapy also reduces inflammatory cytokines. Inflammation plays a significant role in hearing damage, particularly in the hours and days following acoustic trauma or other injuries.
By dampening the inflammatory response, photobiomodulation may prevent secondary damage that occurs after the initial insult.
Additionally, photobiomodulation modulates apoptotic pathways. Apoptosis is programmed cell death, a process that cells undergo when they’re damaged beyond repair.
In some cases, cells that could potentially recover instead trigger apoptosis prematurely.
Red light therapy appears to inhibit pro-apoptotic signals and enhance pro-survival signals, giving damaged hair cells a better chance of recovering as opposed to dying.
Studies have even shown that photobiomodulation can upregulate genes involved in cellular protection. This means the therapy doesn’t just provide immediate benefits during treatment but can trigger longer-lasting changes in how cochlear cells respond to stress.
The Evidence for Different Types of Hearing Loss
Noise-Induced Hearing Loss
Noise-induced hearing loss has received the most attention in photobiomodulation research. This makes sense because it represents one of the most common forms of preventable hearing damage, affecting millions of people worldwide from occupational exposure, recreational activities, and environmental noise.
Studies in animal models have consistently demonstrated that red light therapy applied shortly after acoustic trauma can significantly reduce the permanent threshold shift that typically occurs.
In laboratory experiments, researchers expose animals to high-intensity noise that would normally cause permanent hearing damage, then treat one group with photobiomodulation while leaving a control group untreated.
The results have been really striking. In some experiments, mice treated with specific wavelengths of near-infrared light showed preservation of up to 50-60% more hair cells compared to untreated controls.
When researchers examined the cochleae under microscopes, the treated animals had noticeably more intact hair cells, better-organized cellular structures, and less inflammatory infiltration.
Functional testing through auditory brainstem responses showed that treated animals had better hearing thresholds across many frequencies. The protective effect was particularly pronounced in the high-frequency range, which is typically the most vulnerable to noise damage.
The timing of treatment appears crucial here. The most dramatic protective effects occur when photobiomodulation is applied within hours of noise exposure, during that critical window when oxidative damage is still progressing.
Some studies have shown benefits even when treatment starts 24-48 hours after exposure, but the effects reduce with longer delays.
This temporal pattern makes sense when you understand the cascade of damage that follows acoustic trauma. The initial mechanical damage to hair cells is followed by hours to days of ongoing injury from reactive oxygen species, excitotoxicity from glutamate release, and inflammatory responses.
Intervening early in this cascade can prevent much of the secondary damage.
This research suggests really practical applications. Musicians who perform loud concerts could receive photobiomodulation treatment immediately afterward.
Industrial workers could use portable light therapy devices at the end of noisy work shifts.
Military personnel could undergo treatment after training exercises involving firearms or explosives. The therapy could become a standard protective intervention after known noise exposures.
Age-Related Hearing Loss
Age-related hearing loss, or presbycusis, represents a different challenge than acute noise damage. This condition develops gradually over decades, involving many mechanisms, including accumulated oxidative damage, reduced cochlear blood flow, loss of neural connections, stiffening of cochlear structures, and metabolic decline in hair cells.
You can’t reverse decades of accumulated damage with a few light treatments. The hair cells that have already died are gone, and photobiomodulation won’t regenerate them.
But there is growing evidence that regular photobiomodulation might help preserve remaining hair cells and potentially slow the progression of age-related hearing decline.
Several studies examining older adults with mild to moderate sensorineural hearing loss have shown modest but measurable improvements in pure-tone thresholds following courses of red light therapy. We’re typically talking about improvements of 5-15 decibels at specific frequencies.
To someone unfamiliar with audiology, that might not sound like much, but for someone struggling to hear conversations in noisy environments, that improvement can make a genuinely meaningful difference in quality of life.
In one study of adults aged 60-75 with mild hearing loss, participants received photobiomodulation treatments three times per week for eight weeks. At the end of the treatment period, roughly 60% showed improvements of at least 10 decibels at one or more frequencies.
The improvements were most common in the mid-frequency range (1000-4000 Hz), which is particularly important for speech understanding.
Follow-up assessments three months after treatment ended showed that some participants maintained their gains while others experienced partial regression. This suggests that ongoing maintenance treatments might be necessary to sustain benefits, similar to how you need to continue exercising to maintain fitness gains.
The mechanisms by which photobiomodulation helps with age-related hearing loss likely involve supporting the metabolic function of remaining hair cells. By enhancing ATP production and reducing oxidative stress, the therapy may help struggling hair cells maintain function that would otherwise decline.
Improved cochlear blood flow could also contribute by ensuring better nutrient delivery to these metabolically demanding cells.
Tinnitus
Tinnitus presents a particularly interesting and complex application for photobiomodulation. The mechanisms underlying phantom sounds are still not fully understood, but research suggests that tinnitus involves both peripheral changes in the cochlea and central changes in how the auditory cortex processes signals.
Some cases of tinnitus appear to involve aberrant neural activity in the auditory cortex, where neurons fire spontaneously in patterns that the brain interprets as sound. Other cases may relate more directly to cochlear damage and altered signaling from the auditory nerve.
Many researchers believe that tinnitus often starts with peripheral cochlear damage but is then maintained by maladaptive plasticity in central auditory pathways.
Research using photobiomodulation for tinnitus has shown mixed results, which probably reflects the heterogeneous nature of the condition. Some patients report a substantial reduction in tinnitus loudness or distress, while others experience no benefit at all.
In clinical studies, typically 30-50% of tinnitus patients experience at least some improvement with photobiomodulation therapy. The improvements range from finish resolution (which is rare) to modest reductions in loudness or changes in the character of the tinnitus that make it less bothersome.
One intriguing finding from several studies is that photobiomodulation seems most effective for tinnitus associated with hearing loss and worst in the higher frequencies. This makes sense if the therapy is primarily working by supporting damaged hair cells and improving cochlear function as opposed to directly modulating central auditory processing.
Patients whose tinnitus is accompanied by measurable high-frequency hearing loss tend to respond better than those with normal audiograms. This suggests that when the tinnitus is linked to identifiable cochlear pathology, treating that pathology can reduce the tinnitus symptoms.
The treatment protocols for tinnitus typically involve longer courses than those used for acute hearing loss. Studies showing positive results usually involved daily or near-daily treatments for at least 8-12 weeks.
Some patients experience a gradual reduction in tinnitus over this period, while others notice more abrupt changes.
Interestingly, some patients report that their tinnitus initially becomes more noticeable during the first week or two of treatment before improving. This phenomenon isn’t well understood but might reflect changes in neural activity or altered attention to the phantom sound.
Treatment Protocols and Technical Considerations
Wavelength Selection
The devil is really in the details when it comes to photobiomodulation parameters. Not all red light is created equal.
The specific wavelength you use significantly impacts how deeply the light penetrates tissue and how strongly it’s absorbed by target chromophores.
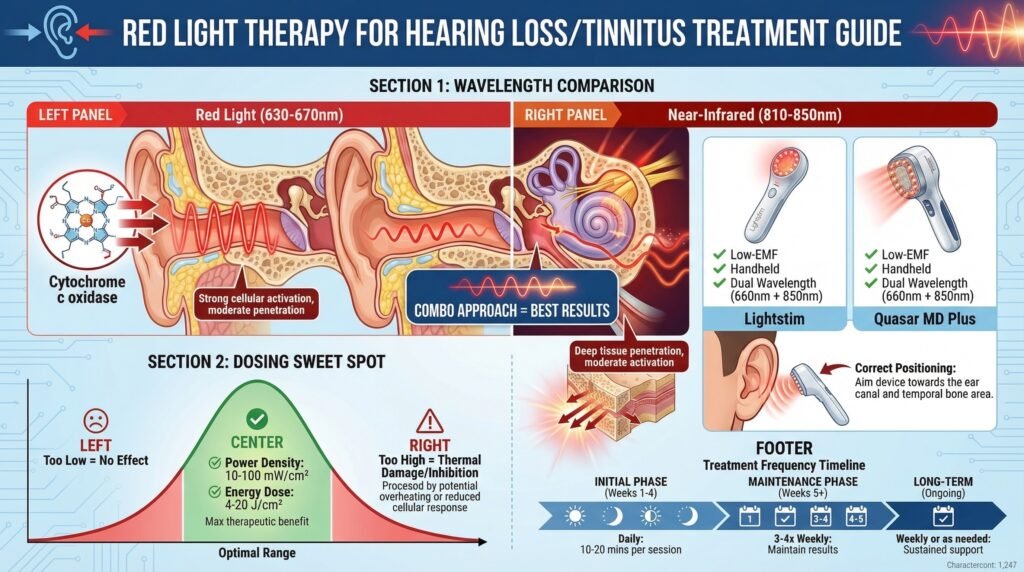
Most successful studies have used wavelengths in the 630-850 nanometer range. Red light around 630-670 nm penetrates reasonably well through tissue but may not reach the deepest structures of the cochlea as effectively as near-infrared wavelengths.
This red light is absorbed strongly by cytochrome c oxidase, which is good for triggering the desired cellular responses.
Near-infrared light around 810-850 nm penetrates deeper into tissue because it’s less absorbed by hemoglobin and water. This gives it better reach to the cochlea, which sits deep within the temporal bone.
However, the absorption by cytochrome c oxidase is somewhat less than with red wavelengths.
Many researchers have found success using a combination approach with dual wavelengths. Some experimental protocols alternate between red and near-infrared in the same treatment session, attempting to get the benefits of both strong chromophore activation and deep tissue penetration.
Power Density and Energy Dose
Power density (measured in milliwatts per square centimeter) determines how much energy reaches the tissue. This parameter is critical because photobiomodulation follows a biphasic dose-response curve.
Too little energy and you won’t achieve therapeutic effects.
Too much and you risk thermal damage or paradoxical inhibition of the processes you’re trying to stimulate.
Most effective protocols use power densities between 10-100 milliwatts per square centimeter. At the lower end of this range, you need longer treatment times to deliver adequate energy.
At the higher end, shorter treatments can deliver sufficient doses, but you must be more careful about heat buildup.
The total energy dose (measured in joules per square centimeter) is the product of power density and treatment time. Successful studies have typically delivered between 4-20 joules per square centimeter per session.
Going below this range tends to produce inconsistent results, while going much above it increases the risk of inhibitory effects without additional benefit.
Best Red Light Therapy Devices for Hearing Loss / Tinnitus
Targeted handheld wands such as the Lightstim and the Quasar MD Plus are affordable, low-EMF devices that can be used for close, focused application to the ear canal and outer ear.
Typically designed for the targeted face and neck treatments, these devices provide the efficacious wavelengths of around 660nm for the surface tissue and near-infrared light of around 850 nm to penetrate deeper into the skin. Read our reviews of the FDA-cleared Lightstim here and the Quasar MD Plus hand-held device here.
>>Click here to buy the Lightstim Handheld Device on Amazon<<
>>Click here to buy the Quasar MD Plus<<
In part 2, we discuss more treatment protocols, combining interventions, and expand on more at-home red light therapy devices you can use to help with treating hearing loss. Follow us for additional updates and educational content.
People Also Asked
Does red light therapy work for tinnitus?
Red light therapy shows promise for some people with tinnitus, particularly when the tinnitus is associated with hearing loss in the higher frequencies. Research studies have found that about 30-50% of tinnitus patients experience at least some improvement with photobiomodulation therapy.
The improvements range from modest reductions in loudness to changes in the character of the tinnitus that make it less bothersome.
Treatment typically needs consistent sessions for 8-12 weeks before determining effectiveness. The therapy appears to work best for tinnitus linked to cochlear damage as opposed to tinnitus that originates primarily from central auditory processing issues.
Can hearing loss from loud noise be reversed?
Permanent hearing loss from loud noise exposure cannot be fully reversed because mammalian hair cells do not regenerate once destroyed. However, there is a critical window immediately following acoustic trauma when intervention may prevent some of the damage from becoming permanent. Red light therapy applied within hours to days of noise exposure has shown the ability to preserve hair cells that would otherwise die, reducing the severity of permanent hearing loss.
The therapy works by interrupting the cascade of oxidative damage and inflammation that continues for hours to days after the initial noise exposure.
For the best results, treatment should begin as soon as possible after the acoustic trauma.
What wavelength of red light is best for hearing?
Most research on photobiomodulation for hearing loss has used wavelengths between 630-850 nanometers. Red light in the 630-670 nm range is absorbed strongly by cellular chromophores but penetrates less deeply through tissue and bone.
Near-infrared light in the 810-850 nm range penetrates more deeply, potentially reaching the cochlea more effectively, though it’s absorbed somewhat less strongly.
Many researchers have found that combining both red and near-infrared wavelengths provides the best results by leveraging both strong chromophore activation and deep tissue penetration. The optimal wavelength may vary depending on person’s ear anatomy and the specific type of hearing loss being treated.
How long does it take for red light therapy to improve hearing?
The timeline for potential hearing improvement with red light therapy varies considerably depending on the type and severity of hearing loss. For acute noise-induced damage, protective effects may be measurable within days to weeks when treatment begins shortly after exposure.
For chronic conditions like age-related hearing loss or tinnitus, most studies showing benefits have used treatment protocols lasting 8-12 weeks with many sessions per week.
Some people notice subjective improvements in hearing or tinnitus within 4-6 weeks, while others need longer treatment courses. Measurable changes on audiometry typically appear after at least 8 weeks of consistent treatment.
For chronic conditions, maintenance treatments may be needed to sustain benefits. See the link below to explore a highly effective red light therapy option for home use.
This article includes affiliate links. If you click through and make a purchase, I may receive a small commission. This helps support the site and allows me to keep creating helpful content at no extra cost to you.